The Plantar Fascia: More Than Just Arch Support
Plantar heel pain is one of the most common musculoskeletal problems affecting the foot. It is frequently seen in runners, people who spend long periods standing at work, and individuals whose activity levels have changed recently. In many cases the symptoms appear gradually rather than following a single identifiable injury. Patients often describe discomfort beneath the heel that is particularly noticeable during the first steps in the morning or after periods of rest.
In everyday explanations the plantar fascia is often described simply as a band of tissue that supports the arch of the foot. While this description is partly true, it does not fully reflect how the plantar fascia behaves during walking and running. The fascia does not just hold the arch up like a passive strap. It helps the foot manage load, store energy, and direct force during movement.
When we walk or run, the foot must deal with substantial forces generated by body weight and forward motion. These forces are not handled by one structure alone. Instead, they are shared across multiple tissues that work together as a load-sharing system. The plantar fascia is an important part of that system.
As body weight is applied to the foot, the arch deforms slightly, stretching the plantar fascia and generating tension within its collagen fibres. This allows the fascia to contribute to force distribution and to the storage and return of mechanical energy during locomotion. However, the plantar fascia does not act alone here. The calf muscles, intrinsic foot muscles, and other soft tissues also help control stiffness and load as the body moves over the foot.
To do this job well, the foot has to perform a sequence of mechanical tasks. First, it must absorb load when the foot contacts the ground. Second, as body weight moves forward, the arch gradually stiffens so the foot can act as a stable lever. Finally, during push-off, the foot directs propulsive force through the forefoot, typically through the first ray and hallux.
These three mechanical functions — absorbing load, increasing stiffness, and directing propulsion — provide a useful way to understand how the foot behaves during movement and why certain tissues may become overloaded when the system is not working well.
Understanding the plantar fascia as part of this load-sharing system gives us a clearer explanation of why plantar heel pain develops and why treatment often focuses on restoring the tissue’s ability to tolerate load rather than simply trying to eliminate activity.
Key Concept Box
The plantar fascia is more than arch support.
It helps the foot:
• absorb load
• stiffen progressively during stance
• store and return some mechanical energy
• help direct propulsion through the medial forefoot and hallux
Symptoms can develop when repetitive loading exceeds the tissue’s current tolerance.
The Windlass Mechanism
One of the most widely taught explanations of plantar fascia function is the windlass mechanism, first described by Hicks in 1954 (1). The term “windlass” refers to a mechanical device used to wind a rope or cable around a drum in order to generate tension.
In the foot, a similar process occurs during the later stages of walking. As the heel lifts from the ground, the toes begin to dorsiflex. When the big toe extends, the plantar fascia wraps around the metatarsal head in a manner similar to a rope winding around a pulley. This increases tension within the fascia, shortens the distance between the heel and the forefoot, and contributes to midfoot stiffness.
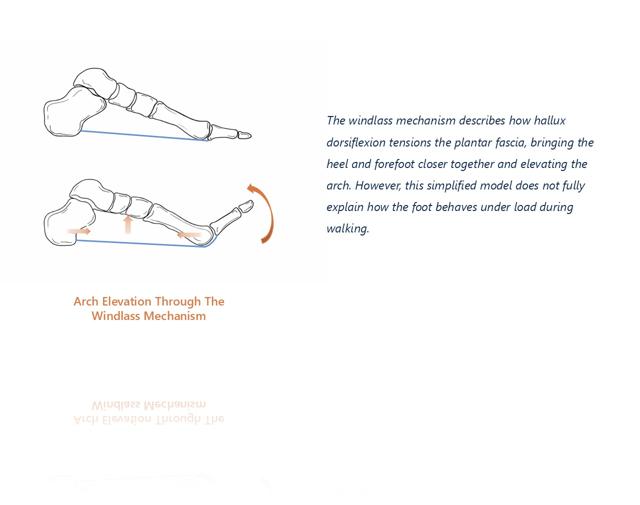
The windlass mechanism helps the foot transition from a relatively flexible structure during early stance to a stiffer lever during push-off. This allows forces generated by the calf muscles to be transmitted efficiently through the forefoot and into the ground.
It is an elegant explanation of how the foot stiffens during propulsion and why the plantar fascia is so important to forward movement.
However, while the windlass mechanism describes an important part of plantar fascia behaviour, it does not explain everything. Research has shown that tension within the fascia begins to develop well before the toes dorsiflex (2,3).
That means there is more going on than toe extension alone. To understand this, we need to look at how the arch behaves when body weight is applied to the foot.
Arch Deflection and Elastic Energy Storage
When the foot first contacts the ground during walking, body weight is transferred onto the arch. The medial longitudinal arch is not rigid, but behaves more like a flexible beam that can deform slightly under load (4).
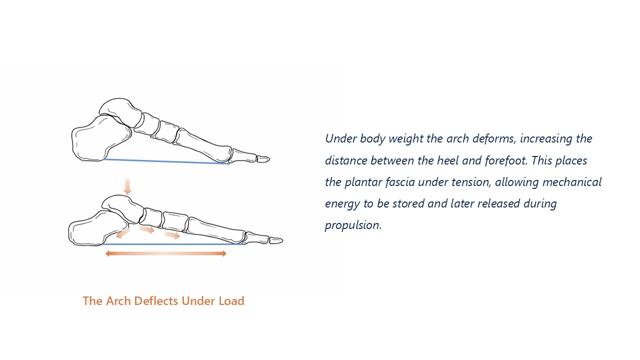
As the arch deflects, the distance between the calcaneus and the metatarsal heads increases. Because the plantar fascia spans this distance, arch deformation stretches the fascia and generates tension within its fibres.
This tension allows the plantar fascia to function as part of an energy-storing system within the foot (5,6). When the fascia elongates, mechanical energy is temporarily stored within the tissue. Later in the gait cycle, as the heel rises and the arch recoils, some of this stored energy can be returned to assist propulsion.
This is similar to the way a spring stores and releases energy when compressed and then allowed to recoil. Early biomechanical studies suggested that the arch of the human foot behaves in a comparable way, helping improve the efficiency of locomotion by recycling mechanical energy.
More recent research using motion analysis and modelling techniques has supported the idea that arch recoil contributes meaningfully to propulsion (7,8). During heel rise the arch can shorten rapidly, releasing stored energy that assists forward movement. Importantly, this recoil is not explained by toe dorsiflexion alone. The windlass mechanism contributes to the process, but it is only one part of a broader mechanical system.
This helps improve the efficiency of walking and running by reducing the amount of active muscular work required for propulsion. However, the ability of the plantar fascia to tolerate these repeated cycles of stretching and recoil depends on the microscopic organisation of the tissue itself.
Mechanical Driver
The main mechanical driver of plantar fascia overload is repeated tensile loading within a system that is also exposed to compression and shear.
As the arch deflects under body weight, the plantar fascia is stretched between the calcaneus and the forefoot. That increases tensile demand within the tissue. At the same time, the heel fat pad, plantar soft tissues, and bony architecture are all contributing to how force is absorbed and redirected through the foot.
In other words, symptoms are not usually driven by one single event. They are more often the result of repeated loading cycles that the fascia is asked to manage over time. When those cycles become more demanding than the tissue is ready for, irritation and structural change can follow.
Several common situations can increase that demand:
- a sudden increase in standing or walking volume
- an aggressive running progression
- reduced ankle dorsiflexion or altered tibial progression
- footwear or surface changes
- reduced capacity of the intrinsic foot muscles and calf complex
From a clinical perspective, the key issue is not just that the fascia is being loaded, but that it may be being loaded in a way, or at a rate, that it is not currently prepared to tolerate.
Microstructure of the Plantar Fascia
The plantar fascia is made up mainly of dense bundles of type I collagen fibres (9) arranged along the length of the arch. These collagen fibres give the tissue the tensile strength it needs to resist the substantial forces generated during gait.
The fibres are organised into fascicles that run predominantly from the calcaneus towards the toes. This orientation allows the tissue to transmit tension efficiently along the length of the arch. When tensile forces are applied to the fascia, the fibres align further in the direction of stress, improving the tissue’s ability to resist deformation.
Surrounding the collagen fibres is an extracellular matrix (ECM) made up of water, proteoglycans and other structural molecules. The ECM plays a crucial role in determining how the fascia behaves mechanically. It helps distribute force between collagen fibres and contributes to the viscoelastic properties of the tissue (10).
Viscoelastic materials behave in a time-dependent way. That means the tissue’s response depends not only on how much load is applied, but also on how quickly and how long that load is applied. Under sustained tension the fascia may gradually elongate, while under rapid loading it behaves more stiffly.
Water content within the ECM also influences tissue mechanics. Proteoglycans attract water molecules, helping maintain hydration within the tissue and supporting its ability to resist compressive forces.
Another important component of fascial tissue is hyaluronic acid, which contributes to lubrication between adjacent layers of connective tissue. Hyaluronic acid helps tissues glide more smoothly during movement (11), reducing friction and allowing adjacent structures to move relative to one another.
Taken together, these structural components allow the plantar fascia to tolerate repeated cycles of loading and unloading during weight-bearing. The combination of strong collagen fibres and a hydrated extracellular matrix enables the tissue to store and release mechanical energy while maintaining structural integrity.
However, the plantar fascia does not function in isolation. It is linked with several other structures in the foot that help distribute mechanical forces.
Structural Integration with the Foot
The plantar fascia is closely integrated with surrounding tissues through a network of fibrous septae that extend from the fascia into the heel and forefoot fat pads. These septae anchor the fat pads to the underlying bones and help stabilise them during weight-bearing (12).
This matters because the plantar surface of the foot is not made up of one simple layer of tissue. It is a layered system, with each part helping the others manage pressure, shear and deformation. The heel fat pad helps absorb impact when the heel contacts the ground, while the forefoot fat pads help distribute load during push-off.
The fibrous connections between the plantar fascia and these fat pads help hold the cushioning system in place. That means the fascia is not just spanning the arch in isolation; it is part of a wider structure that helps the foot cope with repeated loading.
These connections also explain why changes in one part of the system can affect the others. If the fascia becomes irritable, or if the fat pad loses some of its normal support, load distribution across the plantar surface can change.
So although the plantar fascia is often discussed on its own, it really behaves as part of a broader mechanical network linking the rearfoot, midfoot and forefoot.
This network also has a sensory role.
Sensory Function of the Plantar Fascia
In addition to its mechanical role, the plantar fascia contains sensory nerve endings that contribute to the detection of mechanical loading within the foot. Studies examining fascial tissues have identified various types of sensory receptors within these structures.
These receptors provide information about pressure and tension within the fascia. That feedback helps the nervous system monitor how forces are being applied to the foot during gait.
Although the sensory role of the plantar fascia is still being explored, it highlights an important point: the fascia is not simply a passive structure. Alongside its mechanical role, it also appears to contribute to sensory feedback within the foot.
By detecting changes in tension or pressure within the fascia, the nervous system can adjust muscle activation patterns to help manage loading through the foot. This sensory feedback is thought to help coordinate muscle activity and maintain stability during movement.
This is one of the reasons the plantar fascia should be thought of as part of a living, responsive system rather than just a sheet of connective tissue.
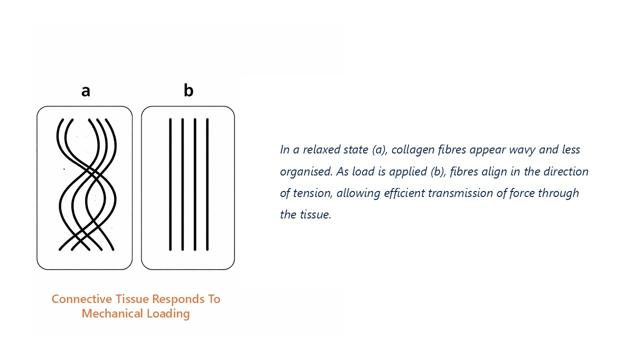
Mechanical Adaptation of Connective Tissue
Connective tissues such as fascia, tendons and ligaments adapt to the mechanical environment in which they function (15,16). When tissues are exposed to repeated mechanical loading, cells within the tissue respond by altering the structure of the extracellular matrix (15,16).
Fibroblasts play a central role in this process. When exposed to mechanical strain, these cells increase the production of collagen and other matrix components. Over time this can lead to structural changes that improve the tissue’s ability to tolerate load.
One important part of this adaptation is collagen alignment along the direction of tensile stress (17). When tissues are regularly loaded in a particular direction, collagen fibres tend to organise themselves along that line of force. This alignment allows the tissue to resist tension more effectively.
At the same time, the extracellular matrix may undergo remodelling that changes the mechanical properties of the tissue. Changes in collagen cross-linking, water content and matrix composition can all influence how the tissue behaves under load.
[Image 3 placeholder: Connective tissue responds to mechanical loading]
This is what makes connective tissue so remarkable. It is not fixed. It adapts to the demands placed on it. Over time it can become better suited to the work it is being asked to do.
This adaptation is not instant, though. When the demands on the tissue rise faster than it can adapt, symptoms are more likely to develop. The issue is not simply that the tissue is being loaded. It is that the loading has outpaced its current tolerance.
That balance becomes especially important when looking at different types of force acting on the fascia.
Tension and Compression in Plantar Fascia Loading
During walking and running the plantar fascia is exposed to multiple types of mechanical forces. The most obvious is tensile loading, which occurs when the arch deflects and the fascia stretches between the heel and the forefoot.
However, the fascia may also experience compressive forces, particularly near its insertion on the calcaneus (18). In this region the fascia lies close to the underlying bone and is subjected to compressive stress during weight-bearing.
Different loading environments can influence how connective tissues adapt. Tensile loading tends to promote collagen alignment along the direction of stress, while compressive environments encourage different cellular responses.
These mechanical differences help explain why certain regions of the plantar fascia are more vulnerable to injury. Areas exposed to both tensile and compressive forces experience complex loading patterns that challenge the tissue’s ability to adapt.
Understanding how different forces act on the fascia gives us another piece of the picture when thinking about plantar heel pain. When these loading patterns are greater than the tissue can handle over time, symptoms begin to develop.
Why Plantar Fascia Injury Develops
Plantar heel pain is now generally considered to involve degenerative changes within the fascia rather than purely inflammatory processes (19,20). Histological studies of affected tissues have demonstrated collagen disorganisation, changes within the extracellular matrix and reduced mechanical integrity of the tissue (19,20).
These changes are often associated with repetitive mechanical loading over time (21). During weight-bearing activities the plantar fascia may experience thousands of loading cycles each day. The tissue is capable of adapting to those forces, but problems can arise if the rate of loading exceeds its ability to recover and remodel.
Several factors influence this balance, including sudden increases in activity levels, changes in footwear, prolonged standing or reduced recovery between loading cycles. When these factors combine, the cumulative load placed on the fascia gradually increases.
As the tissue becomes less able to tolerate those forces, structural changes occur within the tissue. Over time these changes reduce the mechanical efficiency of the fascia and lead to the development of symptoms.
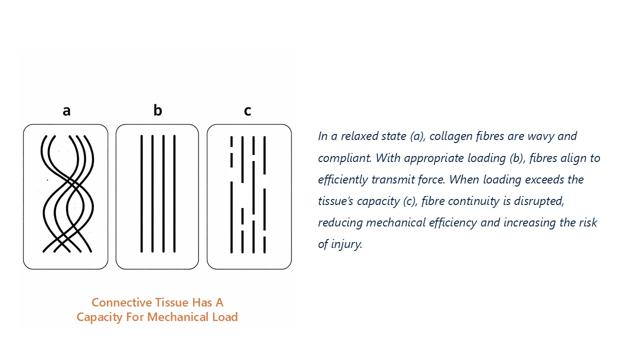
Load vs Capacity and Rehabilitation
A useful way to understand many musculoskeletal injuries is through the relationship between mechanical load and tissue capacity.
Mechanical load refers to the forces applied to a tissue during activities such as walking, running or standing. Tissue capacity refers to the ability of that tissue to tolerate those forces.
When mechanical load repeatedly exceeds tissue tolerance, structural changes and pain may develop. This imbalance rarely happens as a single event. More commonly it develops gradually as the demands on the tissue rise over time.
Treatment therefore aims to restore balance between these two factors. That may involve temporarily reducing mechanical load while gradually improving the tissue’s ability to tolerate stress.
Rehabilitation often focuses on progressive loading strategies designed to stimulate tissue adaptation while avoiding excessive strain. Strengthening exercises, movement retraining and appropriate load management can all contribute to improving tissue capacity.
In some cases orthoses may also be used to modify how forces are distributed through the foot. Rather than acting as passive supports, orthoses function as load-modulation tools, altering how mechanical stress is applied to tissues during movement.
[Image 4 placeholder: Connective tissue has a capacity for mechanical load]
By improving the balance between load and tissue capacity, rehabilitation aims to restore the plantar fascia’s role within the foot’s load-sharing and energy-storing system.
Clinical Takeaway
Plantar heel pain is not simply a problem of “tight fascia” or “poor arch support.”
It is better understood as a load-management problem involving repeated tensile demand on a tissue that may not currently have enough tolerance to handle it.
That means the most useful clinical questions are not only:
- where is the pain?
- but also:
- what is the tissue being asked to do?
- how is it being loaded?
- why is that load concentrated there?
- and does the tissue currently have enough tolerance to cope?
That framework helps explain both the cause of symptoms and the logic behind treatment.
Summary
The plantar fascia is often described as a simple structure supporting the arch of the foot. In reality it plays a far more dynamic role in the mechanics of walking and running.
During weight-bearing the arch of the foot deflects slightly under load, stretching the plantar fascia and generating tension within its collagen fibres. This process allows the fascia to store elastic energy within the arch, which can later be released during heel rise to assist propulsion.
The familiar windlass mechanism explains how the fascia tightens as the toes dorsiflex during push-off, contributing to midfoot stiffness. However, research suggests that the plantar fascia begins to experience substantial loading much earlier in the stance phase as the arch deforms under body weight.
The mechanical behaviour of the plantar fascia is closely linked to its microscopic structure. Dense bundles of collagen fibres, supported by a hydrated extracellular matrix, allow the tissue to tolerate repeated cycles of stretching and recoil during walking and running. Connections between the fascia and surrounding structures, including the heel and forefoot fat pads, also help distribute forces across the plantar surface of the foot.
Like other connective tissues, the plantar fascia adapts to the mechanical environment in which it functions. When exposed to appropriate levels of loading, collagen fibres align along the direction of stress and the tissue becomes better able to tolerate mechanical forces. However, if the demands placed on the tissue rise faster than it can adapt, structural changes may occur within the fascia.
From this perspective plantar heel pain can be understood as a problem within the foot’s load-management system. Repetitive loading, insufficient recovery or changes in activity levels may gradually shift the balance between mechanical load and tissue tolerance.
Effective treatment therefore focuses not only on reducing painful loading but also on restoring the ability of the plantar fascia to tolerate mechanical stress. Rehabilitation strategies that gradually reintroduce load help stimulate tissue adaptation and improve the resilience of the system.
Understanding the plantar fascia as part of a dynamic load-sharing and energy-storing system provides a clearer framework for both the development and treatment of plantar heel pain.
References
(1) Hicks JH. The mechanics of the foot. II. The plantar aponeurosis and the arch. J Anat. 1954.
(2) Carlson RE et al. The role of the plantar aponeurosis in arch support. Foot Ankle Int. 2000.
(3) Erdemir A et al. An elaborate data set characterizing the mechanical response of the foot. J Biomech. 2004.
(4) Ker RF et al. The spring in the arch of the human foot. Nature. 1987.
(5) Ker RF. Mechanics of the foot and ankle. Clin Sports Med. 1998.
(6) Wearing SC et al. The pathomechanics of plantar fasciitis. Sports Med. 2006.
(7) Zelik KE, Honert EC. Ankle and foot power in walking and running. J Biomech. 2018.
(8) Kelly LA et al. Intrinsic foot muscles contribute to arch stiffness. J R Soc Interface. 2014.
(9) Benjamin M. The fascia of the limbs and back. J Anat. 2009.
(10) Fung YC. Biomechanics: Mechanical Properties of Living Tissues. 1993.
(11) Stecco C et al. The role of fascia in movement and proprioception. J Bodyw Mov Ther. 2014.
(12) Wearing SC et al. Plantar fat pad structure and function. J Anat. 2009.
(13) Schleip R. Fascial plasticity and mechanoreception. J Bodyw Mov Ther. 2003.
(14) Yahia LH et al. Sensory innervation of fascia. Acta Orthop Scand. 1992.
(15) Kjaer M. Role of extracellular matrix in adaptation. Physiol Rev. 2004.
(16) Magnusson SP et al. Viscoelastic response to loading. J Physiol. 2008.
(17) Wang JH. Mechanobiology of connective tissue. J Biomech. 2006.
(18) Benjamin M et al. Entheses and tendon-bone interface. J Anat. 2006.
(19) Lemont H et al. Plantar fasciitis: degenerative process. J Am Podiatr Med Assoc. 2003.
(20) Maffulli N et al. Tendinopathy model (degenerative paradigm). Clin Sports Med. 2003.
(21) Li J, Muehleman C. Histopathology of plantar fasciitis. Foot Ankle Int. 2007.